
Surgery
What patients need to know

Is surgery an option for people with advanced lung cancer?
More and more people living with stage IV oncogene-driven lung cancer are asking whether surgery might be an option — especially when targeted therapies lead to strong responses. But currently, there are no patient-facing guidelines worldwide. In the UK, conversations around surgery in advanced lung cancer often aren’t likely to be initiated by clinical teams.
This section was co-developed with patient advocates, medical patient advisors, and thoracic surgeons to help people understand when surgery might be considered in advanced lung cancer — and to support informed discussions with your care team.
What to know about surgery and local treatment options in the advanced lung cancer setting.
Research shows that for some people with stage IV non-small cell lung cancer (NSCLC), treating all the sites of disease with surgery and/or radiotherapy may help them live longer. With careful selection, combining drug treatment with local surgery or radiotherapy, as part of a team approach, is becoming an important option for controlling the disease and improving survival.
While international expert bodies like ASCO, ASTRO, ESMO, ESTRO and The Society of Thoracic Surgeons (STS) now recognise that local consolidative therapy (LCT) – including surgery – is recommended for carefully selected patients with advanced lung cancer, no dedicated, plain-language patient guidelines currently exist to help understand what this means.
Here we provide clear, accessible information to help you understand surgical local consolidative therapy options and empower you to participate in informed discussions with your care teams.
Standard of care in stage IV lung cancer
Historically, stage IV lung cancer has been treated with chemotherapy, radiotherapy, immunotherapy and targeted therapy. People with oncogene-driven lung cancers often have better options for controlling the main tumour (and some spread) with targeted drugs. Local therapies — surgery or radiation — are currently used to tackle sites of cancer progression and/or stable disease sites. By utilising these local therapies, people often can remain on their current targeted drug after such treatment.
Despite the efficacy of therapies currently used to treat oncogene-driven NSCLC, cancer research has shown that there is usually persistence of disease within the original site. This can result in the cancer becoming active again and potentially spreading to more tumour cells. Removal of this site may improve survival.
Questions patients often ask about surgery in stage IV lung cancer
1. Can surgery treat my lung tumour and nodes at stage IV?
Clinical trials show that for oncogene-driven lung cancers, surgery or radiotherapy can remove or treat the main lung tumour and sometimes chest lymph nodes near the tumour site, as well as a few distant spots. Common sites for surgical removal include the adrenal gland and, less commonly, the liver. Brain metastases are usually treated with focused radiation (not open surgery), but rarely, surgery may be used for a single accessible brain tumour.
Tissue removed at surgery will be tested to see if it contains cancer cells and identify if the cancer cells may still be active. Patients are advised to remain on their targeted therapy after surgery. In all cases, these decisions depend on careful staging and teamwork with your cancer specialists.
2. Is there any research on the use of surgery in people with oncogene-driven lung cancer?
Research studies like NORTHSTAR, BRIGHTSTAR, and LONESTAR are testing how surgery or precise radiation can work with targeted drugs for people with EGFR and ALK mutations, and also for people receiving immunotherapy. These trials look at whether adding local treatment can help people stay on their targeted therapy longer and live well for more time.
3. What do the UK NICE guidelines say about surgery for stage IV lung cancer?
In the UK, the NICE (National Institute for Health and Care Excellence) guidelines focus on drug treatments and radiotherapy for disease with distant spread. This may change in future when the results of the research trials noted above are available. Currently, surgery is usually only offered from stage I to IIIA in selected people, depending on willingness and fitness for surgery. They do not specifically recommend surgery for stages IIIB, IIIC and IV disease. Any surgery for these cases should be discussed with a specialist team.
Download our full Patient Info guide here.

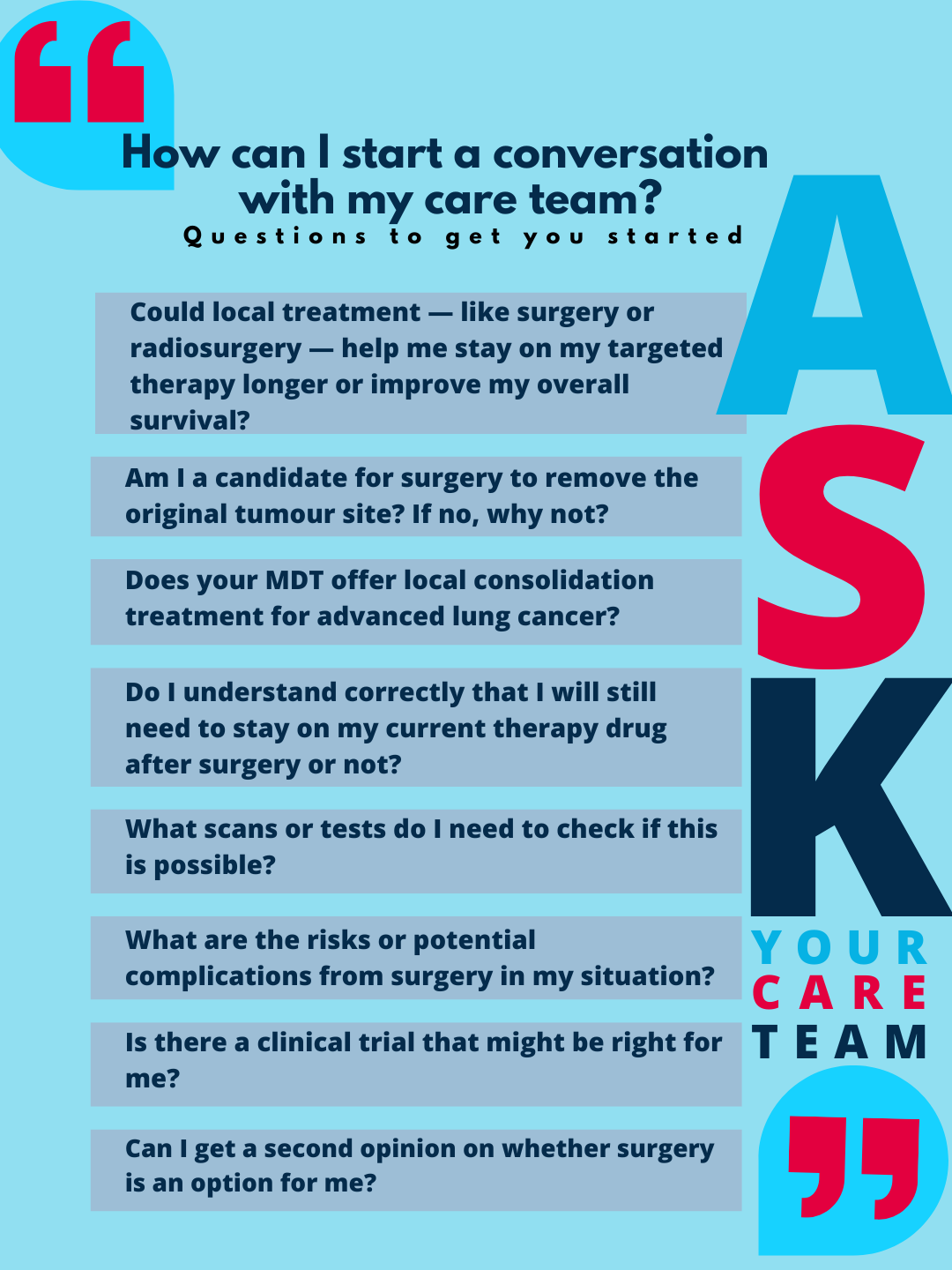
How do I start a conversation with my care team?
Oncogene Cancer Research does not provide medical advice. Always talk to your care team about what’s right for you. Knowledge gives you options and the power to participate in your care decisions. This information was co-developed with our medical patient advisors and reviewed by our thoracic surgeon advisors.
Industry guidelines:
Society of Thoracic Surgeons’ (STS) has updated guidelines for professionals [behind a paywall]. There are no official patient guidelines yet. This open access paper on surgical management is a helpful resource as is this patient friendly page on Professor Eric Lim’s website.
Real questions. Real stories.
Surgery is personal. Here we will feature patients who pushed for answers — and options. Read their inspiring stories.
-

Fighting for surgery: Steve’s stage IV story
Told surgery wasn’t an option, Steve—a molecular biologist living with ALK+ lung cancer—refused to accept that answer. Drawing on his scientific background, he pushed for a second opinion and waited nearly two years to undergo the surgery he believed could help. His story is one of persistence, hope, and the critical importance of informed discussions between patients and care teams.